THE RESPIRATORY SYSTEM
When you take a breath in and then breathe out, you are using both your respiratory and circulatory systems to handle the oxygen you take in. This is called respiration. The processes of respiration give oxygen (O2) to the body and get rid of carbon dioxide (CO2). It is more important to get rid of the CO2 than to get O2 into the body because more CO2 means a shifted pH. This off-sets a lot of internal chemistry and is lethal.
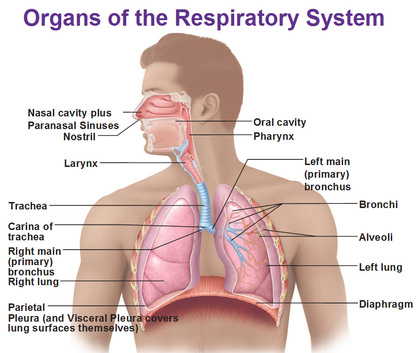
The main organs of the respiratory system are the nose, nasal cavity, paranasal sinuses, pharynx (just below tongue attachment, ABOVE the larynx), larynx, trachea, bronchi, lungs, and alveoli (at end of the bronchi). Refer to the image to the left.
The nose functions as an airway for respiration, moistens the air that we take in, filters air with nose hairs and particle-trapping mucus, and has little receptors in the back of the cavity that allow you to smell! Have you ever wondered what the two lines were above your upper lip and below your nostrils? Those lines make up the "philtrum" of your nose. Another interesting thing to note about the nose is that the cavity is BEHIND it as opposed to ABOVE it. Most people believe the nostrils lead straight up, whereas they really lead straight back into the nasal sinus. If you look at the nasal cavity on the image, you will see 3 flap-like structures. These are the conchae. These help to do the filtering, warming, and moisturizing of the air you breathe in. Pretty cool huh? This is why it can be beneficial to dedicated runners (running in the cold) to breathe through th
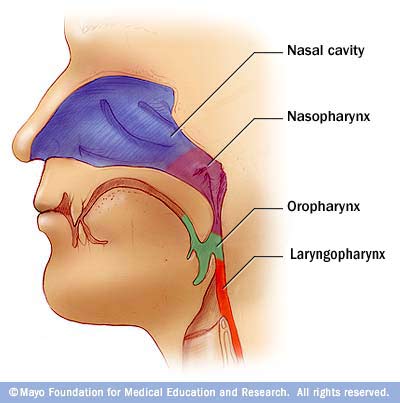
The nasopharynx of our respiratory anatomy is the space in the system that holds the uvula--the thing hanging from the roof of your mouth that you see when you say "ah". In the nasopharynx, there is also the pharyngeal tonsil (adenoids) and the pharyngotympanic tube (eustachian) orifices that help to equalize pressure in the middle ear and throat.
The oropharynx is the space in between the soft palate of the nasopharynx to the epiglottis (flap that folds down over your trachea when you swallow down your esophagus). The palatine tonsils are housed here (these are the ones you can see when you say "ah", one on each side). Some people have more prominent palatine tonsils which is a reason some children have them taken out. They can grow to be big enough to obstruct airflow/swallowing through the mouth. In the oropharynx, the epithelium changes to stratified squamous epithelium as to provide more protection to tissues with abrasive swallowing activity it must endure. Below the oropharynx is the laryngopharynx. This structure is the pathway for both and air before they separate into the esophagus and the trachea. It is continuous with the esophagus as it moves downward.
The larynx comes next. This is the place where that special bone is found, the hyoid bone--the only free floating bone (without any articulations) in the human body. It is the place of VOICE PRODUCTION. Most importantly, the larynx houses the vocal cords (made up of elastic fibers that form vocal folds). Between these cords is the glottis opening. How is sound made exactly? There are muscles that cooperate to create your voice; these are the muscles of the pharynx, tongue, soft palate, and lips. The larynx is continuous with the trachea.
The main organs of the respiratory system are the nose, nasal cavity, paranasal sinuses, pharynx (just below tongue attachment, ABOVE the larynx), larynx, trachea, bronchi, lungs, and alveoli (at end of the bronchi). Refer to the image to the left.
The nose functions as an airway for respiration, moistens the air that we take in, filters air with nose hairs and particle-trapping mucus, and has little receptors in the back of the cavity that allow you to smell! Have you ever wondered what the two lines were above your upper lip and below your nostrils? Those lines make up the "philtrum" of your nose. Another interesting thing to note about the nose is that the cavity is BEHIND it as opposed to ABOVE it. Most people believe the nostrils lead straight up, whereas they really lead straight back into the nasal sinus. If you look at the nasal cavity on the image, you will see 3 flap-like structures. These are the conchae. These help to do the filtering, warming, and moisturizing of the air you breathe in. Pretty cool huh? This is why it can be beneficial to dedicated runners (running in the cold) to breathe through th
The nasopharynx of our respiratory anatomy is the space in the system that holds the uvula--the thing hanging from the roof of your mouth that you see when you say "ah". In the nasopharynx, there is also the pharyngeal tonsil (adenoids) and the pharyngotympanic tube (eustachian) orifices that help to equalize pressure in the middle ear and throat.
The oropharynx is the space in between the soft palate of the nasopharynx to the epiglottis (flap that folds down over your trachea when you swallow down your esophagus). The palatine tonsils are housed here (these are the ones you can see when you say "ah", one on each side). Some people have more prominent palatine tonsils which is a reason some children have them taken out. They can grow to be big enough to obstruct airflow/swallowing through the mouth. In the oropharynx, the epithelium changes to stratified squamous epithelium as to provide more protection to tissues with abrasive swallowing activity it must endure. Below the oropharynx is the laryngopharynx. This structure is the pathway for both and air before they separate into the esophagus and the trachea. It is continuous with the esophagus as it moves downward.
The larynx comes next. This is the place where that special bone is found, the hyoid bone--the only free floating bone (without any articulations) in the human body. It is the place of VOICE PRODUCTION. Most importantly, the larynx houses the vocal cords (made up of elastic fibers that form vocal folds). Between these cords is the glottis opening. How is sound made exactly? There are muscles that cooperate to create your voice; these are the muscles of the pharynx, tongue, soft palate, and lips. The larynx is continuous with the trachea.
The Trachea (also known as the windpipe) is the route our air flows through to get to our lungs. It has muscle called the trachealis muscle that allows us to get rid of mucus in our respiratory system. The trachea split at the carina and then branch into bronchi another 23 times into a tree-like form. The bronchus of the right lung is wider and more vertical than the left lung. Because it is so vertical, more pieces of food and inhaled things are lodged there. When someone has something obstructing their breathing, this is the most common place to find the blocking agent. Talking about the bronchi leads me to discuss the conducting zone. Conducting zones are the "roads" that air takes to get to the respiratory zone, where gas is actually exchanged in the alveoli.
The lungs, which you are probably familiar with, are the main organ of respiration. They are split into the right and left lungs. The left lung is smaller (with 2 lobes compared the right lung's 3 lobes) and even has a special notch to allow room for the heart. Parietal and visceral pleura line the thoracic cavity. Between them is fluid that increases surface tension and helps the lungs stick and expand during inhalation.
The lungs, which you are probably familiar with, are the main organ of respiration. They are split into the right and left lungs. The left lung is smaller (with 2 lobes compared the right lung's 3 lobes) and even has a special notch to allow room for the heart. Parietal and visceral pleura line the thoracic cavity. Between them is fluid that increases surface tension and helps the lungs stick and expand during inhalation.
PULMONARY VENTILATION

Pulmonary ventilation is a fancy phrase for breathing. It includes inhaltion (taking a breath in) and expiration (breathing out). When you breathe, the volume in your abdominal cavity and thoracic cavity change--allowing the movement of gases.
With inspiration, the diaphragm beneath your lungs lengthens as the rib cage expands. As the diaphragm moves down and contracts, the pressure in the thoracic cavity decreases, pulling air from the higher pressure outside of your body into your lungs. "During quiet breathing, the movement of the diaphragm accounts for most of the increase in thoracic volume. The diaphragm is a strong, dome-shaped muscle attached to the body wall around the base of the rib cage. The contraction and flattening of the diaphragm cause a piston-like downward motion that increases the vertical dimension of the chest. Other muscles that participate in breathing are the external and internal intercostal muscles. These muscles run at different angles in two layers between the ribs."
With expiration, the diaphragm shortens and relaxes and the volume of the lungs decreases. The pressure in the thoracic cavity increases and forces air out of the lungs--creating the breathe out motion. "In exhalation, the passive phase of breathing, the respiratory muscles relax, allowing the ribs and diaphragm to return to their original positions. The lung tissues are elastic and recoil to their original size during exhalation. Surface tension within the alveoli aids in this return to resting size. During forced exhalation, the internal intercostal muscles contract, pulling the bottom of the rib cage in and down. The muscles of the abdominal wall contract, pushing the abdominal viscera upward against the relaxed diaphragm. A lung capacity is a sum of volumes. These same values are shown on a graph as they might appear on a tracing made by a spirometer, an instrument for recording lung volumes. The tracing is a spirogram. (link to source at button below)"
With inspiration, the diaphragm beneath your lungs lengthens as the rib cage expands. As the diaphragm moves down and contracts, the pressure in the thoracic cavity decreases, pulling air from the higher pressure outside of your body into your lungs. "During quiet breathing, the movement of the diaphragm accounts for most of the increase in thoracic volume. The diaphragm is a strong, dome-shaped muscle attached to the body wall around the base of the rib cage. The contraction and flattening of the diaphragm cause a piston-like downward motion that increases the vertical dimension of the chest. Other muscles that participate in breathing are the external and internal intercostal muscles. These muscles run at different angles in two layers between the ribs."
With expiration, the diaphragm shortens and relaxes and the volume of the lungs decreases. The pressure in the thoracic cavity increases and forces air out of the lungs--creating the breathe out motion. "In exhalation, the passive phase of breathing, the respiratory muscles relax, allowing the ribs and diaphragm to return to their original positions. The lung tissues are elastic and recoil to their original size during exhalation. Surface tension within the alveoli aids in this return to resting size. During forced exhalation, the internal intercostal muscles contract, pulling the bottom of the rib cage in and down. The muscles of the abdominal wall contract, pushing the abdominal viscera upward against the relaxed diaphragm. A lung capacity is a sum of volumes. These same values are shown on a graph as they might appear on a tracing made by a spirometer, an instrument for recording lung volumes. The tracing is a spirogram. (link to source at button below)"
Physical Factors That Influence Breathing (Pulmonary Ventilation)
1. Airway Resistance - Friction, major NONELASTIC source of resistance. This is usually insignificant because the airways of our lungs are wide enough to provide low resistance air movement. Resistance disappears at the terminal bronchioles because diffusion takes over air movement. A good example of airway resistance is an asthma attack, when the airways narrow significantly. Bronchodilators such as albuterol sulfate or fluticasone propionate/salmeterol inhalers helps to widen airways and facilitate full breathing.
2. Alveolar Surface Tension - Surface tension keeps a liquid from spreading and keeps the particles together. Surfactant is a lipid-protein complex that is made by type II alveolar cells (Type I alveolar cells are very thin cells responsible for much of the gas exchange in our alveoli). Type II alveolar cells are made in the human body during the 7th month of development in pregnancy. This is why many pre-term babies have breathing problems--because their lungs didn't have a chance to establish secretory cells that make surfactant. The surfactant reduces surface tension around the alveoli and keeps them from sticking together or collapsing.
3. Lung Compliance - Compliance of your lungs is the measure of the change in their volume during breathing. Basically, it is the ability of your lungs to expand and deflate--or take a good breath. Compliance is usually high because of the lungs elastic nature and because of the alveolar surface tension mentioned above and in the video link below. Scar tissues formed by asbestos entering the lungs can cause fibrosis and decreases the lung compliance (The lungs are not complying to your will to take a deep breath, simply). People with cystic fibrosis also suffer from lack of surfactant, replaced by excessive mucus. Deformities of the spine (scoliosis) and ribs can inhibit proper breathing and paralysis of intercostal muscles can definitely affect the compliance of the lungs to expand for air. SEE THE VIDEO BELOW!
2. Alveolar Surface Tension - Surface tension keeps a liquid from spreading and keeps the particles together. Surfactant is a lipid-protein complex that is made by type II alveolar cells (Type I alveolar cells are very thin cells responsible for much of the gas exchange in our alveoli). Type II alveolar cells are made in the human body during the 7th month of development in pregnancy. This is why many pre-term babies have breathing problems--because their lungs didn't have a chance to establish secretory cells that make surfactant. The surfactant reduces surface tension around the alveoli and keeps them from sticking together or collapsing.
3. Lung Compliance - Compliance of your lungs is the measure of the change in their volume during breathing. Basically, it is the ability of your lungs to expand and deflate--or take a good breath. Compliance is usually high because of the lungs elastic nature and because of the alveolar surface tension mentioned above and in the video link below. Scar tissues formed by asbestos entering the lungs can cause fibrosis and decreases the lung compliance (The lungs are not complying to your will to take a deep breath, simply). People with cystic fibrosis also suffer from lack of surfactant, replaced by excessive mucus. Deformities of the spine (scoliosis) and ribs can inhibit proper breathing and paralysis of intercostal muscles can definitely affect the compliance of the lungs to expand for air. SEE THE VIDEO BELOW!
Respiratory volumes & capacities
If you've ever had a check up for asthma, or a visit with the doctor for upper respiratory infections, you've most likely blown into a device that measures what you exhale. This type of test is measuring something to do with respiratory volume. It's used to detect any problems your lungs have or to check to make sure they are healthy. Different kinds of volumes include tidal volume (TV), inspiratory reserve volume (IRV), expiratory reserve volume (ERV), and residual volume (RV). Tidal volume is the volume of air that moves in and out of the lungs within one breath, about 500 ml. IRV is the volume of air that you can inhale beyond the 500 ml of the tidal volume. Basically, this is a deep deep breath at about 2100 ml! ERV is air that can be evacuated from the lungs beyond the tidal volume, about 1000 to 1200ml! RV is the air left in the lungs after a powerful expiration. This leftover air is interesting because it is what keeps your lungs from collapsing. It kind of just hangs out in your lungs as the backup and support air. For a graphical display of these types of breathing, see below.
Respiratory capacities are a little bit different. They are "collective volumes", so they always include 2 or more combined volumes discussed above. Inspiratory capacity is the total air that can be taken in after tidal inhalation (IRV + TV). Functional residual capacity is the amount of air remaining in the lungs after an expiration (RV + ERV). Vital capacity is the total amount of exchangable air and does NOT include residual capacity (TV + IRV + ERV). Total lung capacity is the combination of all lung volumes. On the chart below, this would stretch from the top to the bottom of the chart.
Respiratory capacities are a little bit different. They are "collective volumes", so they always include 2 or more combined volumes discussed above. Inspiratory capacity is the total air that can be taken in after tidal inhalation (IRV + TV). Functional residual capacity is the amount of air remaining in the lungs after an expiration (RV + ERV). Vital capacity is the total amount of exchangable air and does NOT include residual capacity (TV + IRV + ERV). Total lung capacity is the combination of all lung volumes. On the chart below, this would stretch from the top to the bottom of the chart.

How well are your lungs working?
Pulmonary function tests are what tell us what our lungs can hold and how they're working. Spirometers are frequently used to do this. Spirometry can tell between OPD (obstructive pulmonary disease, increased airway resistance) and restrictive problems that reduce total lung capacity from structural changes as in TB or fibrosis). When you go to the doctor to take one of these tests, it is common that they are measuring your FVC or forced vital capacity. This is the air you breath out with force after taking a deep breath.

gas exchanges between blood, tissues, & lungs
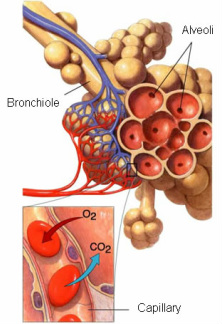
Respiration can either be external (between air, alveoli, to RBC's) or internal (between RBC's and body cells). The alveoli have more CO2 than what is in the atmosphere.
External Respiration occurs between the respiratory membrane which is located between the alveoli and blood supply. There is a higher pressure in the alveoli than there is in the venous blood. This is why the air you take in is transported to the blood from the alveoli, moving down a partial gradient. Two important points:
* A higher O2 level in the alveoli forces O2 to the capillaries.
* A higher CO2 level in the capillaries forces CO2 back to the alveoli to be expelled by the lungs
Ventilation-Perfusion coupling is another important thing to know with external respiration. Ventilation: amount of gas reaching alveoli
Perfusion: amount of blood flow reaching alveoli
When O2 is low or high, this affects the CIRCULATORY SYSTEM (arterioles).
- Low O2, arterioles constrict
- High O2, arterioles dilate
When CO2 is low or high, this affects the RESPIRATORY SYSTEM (bronchioles).
- Low CO2, bronchioles constrict
- High CO2, bronchioles dilate
Internal Respiration
In external respiration, remember that the oxygen concentration was higher in the alveoli than in the capillaries. When you look at internal respiration, the oxygen levels ARE higher in the capillaries, compared to the body cells. This is very important to know!
With internal respiration:
Capillary: High O2, low CO2
Body cell: Low O2, high CO2
Transport of O2: Most oxygen is bound to hemoglobin on the Fe molecule on a RBC. 4 oxygen molecules can bind to RBC along with 1 CO2 molecule. Hemoglobin is what gives blood its bright red color. Hb is released from RBC's when exposed to air, and this decrease of Hb on a RBC is what gives dried blood a darker color. The more O2 that we carry, the more O2 that is put onto RBC's (loading). The more O2 we release, the more our RBC's release it (unloading). Increases of O2 pressures, temperature, pH, pressure of CO2, and concentration of BPG (unloading factor) increase the amount of unloaded oxygen into body tissues. In contrast, when temperature drops or oxygen increases, this encourages loading to happen. Only about 20-25% of oxygen on hemoglobin is unloaded in one circulation of blood. The transport of O2 can be inhibited by having too few red blood cells, too little hemoglobin, blocked circulation, COPD, and carbon monoxide.
Transport of CO2 is a little different. Where oxygen travels mainly on the hemoglobin (98%), only about 20% of CO2 travels on the globin. Most CO2 travels in the plasma as bicarbonate (HCO3-). CO2 first combines with water to form carbonic acid. Most of this happens in the RBC. It then dissociates into HCO3- and H+ ions that make the blood more acidic --> lower ph --> more oxygen released from hemoglobin.
Transport of CO2 in SYSTEMIC capillaries: HCO3- diffuses from RBC's into the plasma. A chloride shift happens where there is an "outrush" of HCO#- from RBC's that is equal to the influx of Cl- moving into the cell from the plasma. Basically, the chloride is replacing the negative charge that was held inside the cell by the bicarbonate (which is now leaving the cell).
Transport of CO2 in PULMONARY capillaries: HCO3- moves INTO RBC's and with a hydrogen ion to make H2CO3 (carbonic acid). H2CO3 is split up by carbonic anhydrase into CO2 & water. CO2 then diffuses into the alveoli.
External Respiration occurs between the respiratory membrane which is located between the alveoli and blood supply. There is a higher pressure in the alveoli than there is in the venous blood. This is why the air you take in is transported to the blood from the alveoli, moving down a partial gradient. Two important points:
* A higher O2 level in the alveoli forces O2 to the capillaries.
* A higher CO2 level in the capillaries forces CO2 back to the alveoli to be expelled by the lungs
Ventilation-Perfusion coupling is another important thing to know with external respiration. Ventilation: amount of gas reaching alveoli
Perfusion: amount of blood flow reaching alveoli
When O2 is low or high, this affects the CIRCULATORY SYSTEM (arterioles).
- Low O2, arterioles constrict
- High O2, arterioles dilate
When CO2 is low or high, this affects the RESPIRATORY SYSTEM (bronchioles).
- Low CO2, bronchioles constrict
- High CO2, bronchioles dilate
Internal Respiration
In external respiration, remember that the oxygen concentration was higher in the alveoli than in the capillaries. When you look at internal respiration, the oxygen levels ARE higher in the capillaries, compared to the body cells. This is very important to know!
With internal respiration:
Capillary: High O2, low CO2
Body cell: Low O2, high CO2
Transport of O2: Most oxygen is bound to hemoglobin on the Fe molecule on a RBC. 4 oxygen molecules can bind to RBC along with 1 CO2 molecule. Hemoglobin is what gives blood its bright red color. Hb is released from RBC's when exposed to air, and this decrease of Hb on a RBC is what gives dried blood a darker color. The more O2 that we carry, the more O2 that is put onto RBC's (loading). The more O2 we release, the more our RBC's release it (unloading). Increases of O2 pressures, temperature, pH, pressure of CO2, and concentration of BPG (unloading factor) increase the amount of unloaded oxygen into body tissues. In contrast, when temperature drops or oxygen increases, this encourages loading to happen. Only about 20-25% of oxygen on hemoglobin is unloaded in one circulation of blood. The transport of O2 can be inhibited by having too few red blood cells, too little hemoglobin, blocked circulation, COPD, and carbon monoxide.
Transport of CO2 is a little different. Where oxygen travels mainly on the hemoglobin (98%), only about 20% of CO2 travels on the globin. Most CO2 travels in the plasma as bicarbonate (HCO3-). CO2 first combines with water to form carbonic acid. Most of this happens in the RBC. It then dissociates into HCO3- and H+ ions that make the blood more acidic --> lower ph --> more oxygen released from hemoglobin.
Transport of CO2 in SYSTEMIC capillaries: HCO3- diffuses from RBC's into the plasma. A chloride shift happens where there is an "outrush" of HCO#- from RBC's that is equal to the influx of Cl- moving into the cell from the plasma. Basically, the chloride is replacing the negative charge that was held inside the cell by the bicarbonate (which is now leaving the cell).
Transport of CO2 in PULMONARY capillaries: HCO3- moves INTO RBC's and with a hydrogen ion to make H2CO3 (carbonic acid). H2CO3 is split up by carbonic anhydrase into CO2 & water. CO2 then diffuses into the alveoli.
CONTROL OF RESPIRATION:

BREATHING INVOLVES NEURONS IN THE BRAIN OF THE RETICULAR FORMATION OF THE MEDULLA AND PONS.
The medullary respiratory center is composed of the Dorsal Root Group (DRG) and the Ventral Respiratory Group (VRG). The DRG keeps our lungs from over-inflating (like a balloon popping) because it has stretch receptors as well as chemoreceptors to regulate breathing. The VRG is special because it is what regulates out breathing rhythm. Inspiratory neurons in this location excite muscles of breathing in the thorax. The Pontine respiratory centers are an extra, believed to be the cause of the pause between an inhalation and exhalation. Beyond this, our complex respiratory rhythm is not well understood except for that it COULD be a cluster of factors.
DEPTH AND RATE OF BREATHING
Depth: determined by how well the respiratory center in the brain works
Rate: determined by how long the inspiratory center is active
Both rate and depth are changed depending on the body's needs. Some interesting chemical factors that influence rate and depth include the influence of CO2. If there is too much CO2 (hypercapnia), then the CO2 combines with water to form carbonic acid, and that dissociates into bicarbonate and H+ ions that increase the acidity and stimulate the chemoreceptors of the brain stem. The decrease in pH is recognized and the brain increases the rate AND depth of breathing to get rid of CO2. Deep breathing--does that remind you of something? It should, especially about hyperventilation. Hyperventilation is the increase of depth and rate of breathing that takes CO2 out of the blood quickly and happens because of hypercapnia (discussed above). Remember it is the not the amount of CO2 that is the true stimulant to the brain, rather it is the amount of H+ ions that decide when you breathe. Hypoventilation is the result of shallow breathing caused by irregular CO2 levels. Sleep apnea is an example of this type of situation, where a person will not breathe until the levels of CO2 rise to the right level. Another chemical factor affecting breathing is oxygen, of course! Oxygen levels, when low, cause the chemoreceptors in the aortic & carotid bodies to be excited and ventilation is then increased.
Reflexes in the Lungs:
1. Irritant reflex = response to an irritant, promote constriction of the bronchioles. In the larger airways, if need be, there are receptors to cause a cough or sneeze to rid the respiratory system from an irritant .
2. Inflation reflex = (Hering-Breuer reflex) Stretch receptors in the pleurae of the lungs are stimuatled when the lungs inflate. There is then a signal sent to stop the inhalation. This reflex protects us from over inflating our lungs, like popping a balloon!
RESPIRATORY ADJUSTMENT:
Exercise: Hyperpnea = increased ventilation. Exercise causes us to need more O2 as well as, most importantly, the ability to rid our bodies of CO2. Because of our awesome adaptations as humans, our CO2 and O2 levels usually remain constant throughout a workout. When you workout, 3 factors in your brain start up as you begin. Psychological stimuli, or thinking about exercising, can prep your body to make changes BEFORE the workout begins. Simultaneous cortical motor activation of skeletal muscles and respiratory centers work together to help you start up and maintain your workout. As exercise comes to an end, ventilation decreases as the brain shuts these things off.
The medullary respiratory center is composed of the Dorsal Root Group (DRG) and the Ventral Respiratory Group (VRG). The DRG keeps our lungs from over-inflating (like a balloon popping) because it has stretch receptors as well as chemoreceptors to regulate breathing. The VRG is special because it is what regulates out breathing rhythm. Inspiratory neurons in this location excite muscles of breathing in the thorax. The Pontine respiratory centers are an extra, believed to be the cause of the pause between an inhalation and exhalation. Beyond this, our complex respiratory rhythm is not well understood except for that it COULD be a cluster of factors.
DEPTH AND RATE OF BREATHING
Depth: determined by how well the respiratory center in the brain works
Rate: determined by how long the inspiratory center is active
Both rate and depth are changed depending on the body's needs. Some interesting chemical factors that influence rate and depth include the influence of CO2. If there is too much CO2 (hypercapnia), then the CO2 combines with water to form carbonic acid, and that dissociates into bicarbonate and H+ ions that increase the acidity and stimulate the chemoreceptors of the brain stem. The decrease in pH is recognized and the brain increases the rate AND depth of breathing to get rid of CO2. Deep breathing--does that remind you of something? It should, especially about hyperventilation. Hyperventilation is the increase of depth and rate of breathing that takes CO2 out of the blood quickly and happens because of hypercapnia (discussed above). Remember it is the not the amount of CO2 that is the true stimulant to the brain, rather it is the amount of H+ ions that decide when you breathe. Hypoventilation is the result of shallow breathing caused by irregular CO2 levels. Sleep apnea is an example of this type of situation, where a person will not breathe until the levels of CO2 rise to the right level. Another chemical factor affecting breathing is oxygen, of course! Oxygen levels, when low, cause the chemoreceptors in the aortic & carotid bodies to be excited and ventilation is then increased.
Reflexes in the Lungs:
1. Irritant reflex = response to an irritant, promote constriction of the bronchioles. In the larger airways, if need be, there are receptors to cause a cough or sneeze to rid the respiratory system from an irritant .
2. Inflation reflex = (Hering-Breuer reflex) Stretch receptors in the pleurae of the lungs are stimuatled when the lungs inflate. There is then a signal sent to stop the inhalation. This reflex protects us from over inflating our lungs, like popping a balloon!
RESPIRATORY ADJUSTMENT:
Exercise: Hyperpnea = increased ventilation. Exercise causes us to need more O2 as well as, most importantly, the ability to rid our bodies of CO2. Because of our awesome adaptations as humans, our CO2 and O2 levels usually remain constant throughout a workout. When you workout, 3 factors in your brain start up as you begin. Psychological stimuli, or thinking about exercising, can prep your body to make changes BEFORE the workout begins. Simultaneous cortical motor activation of skeletal muscles and respiratory centers work together to help you start up and maintain your workout. As exercise comes to an end, ventilation decreases as the brain shuts these things off.
The Mountain climbing experience: how do the lungs hold up?

Ever wonder how mountain climbers stay standing when they're climbing at dangerous altitudes with little oxygen? It's hard to believe, but the human body is amazing enough to accommodate that shift and stay alive! Many mountain climbers take their time when they climb. They often travel in a big group and have a lot of supplies on them--because they know to make a safe ascent they must travel slowly. If you go into high altitudes too fast, your body doesn't have too much time to catch up and it can cause mountain sickness, with headaches, nausea, and shortness of breath. With slow ascent, however, the body will acclimatize. This means that it will adjust to the altitude. When climbing higher, chemoreceptors in our bodies are more responsive to the CO2 in our blood as our O2 content shrivels away. In a few days, breathing will stabilize and we would breathe 2/3 L/min more air than at our home on the ground (sea level). With a lot of practice and training, long term changes will happen in our body. This includes stimulation of the kidneys to make erythropoietin, stimulated by low O2, which makes more RBC's to carry more oxygen! Amazing isn't it?
